Referring Doctor Form
Referring Doctor Form
Referring Doctor Form
Contact Information
Leave Us a Message
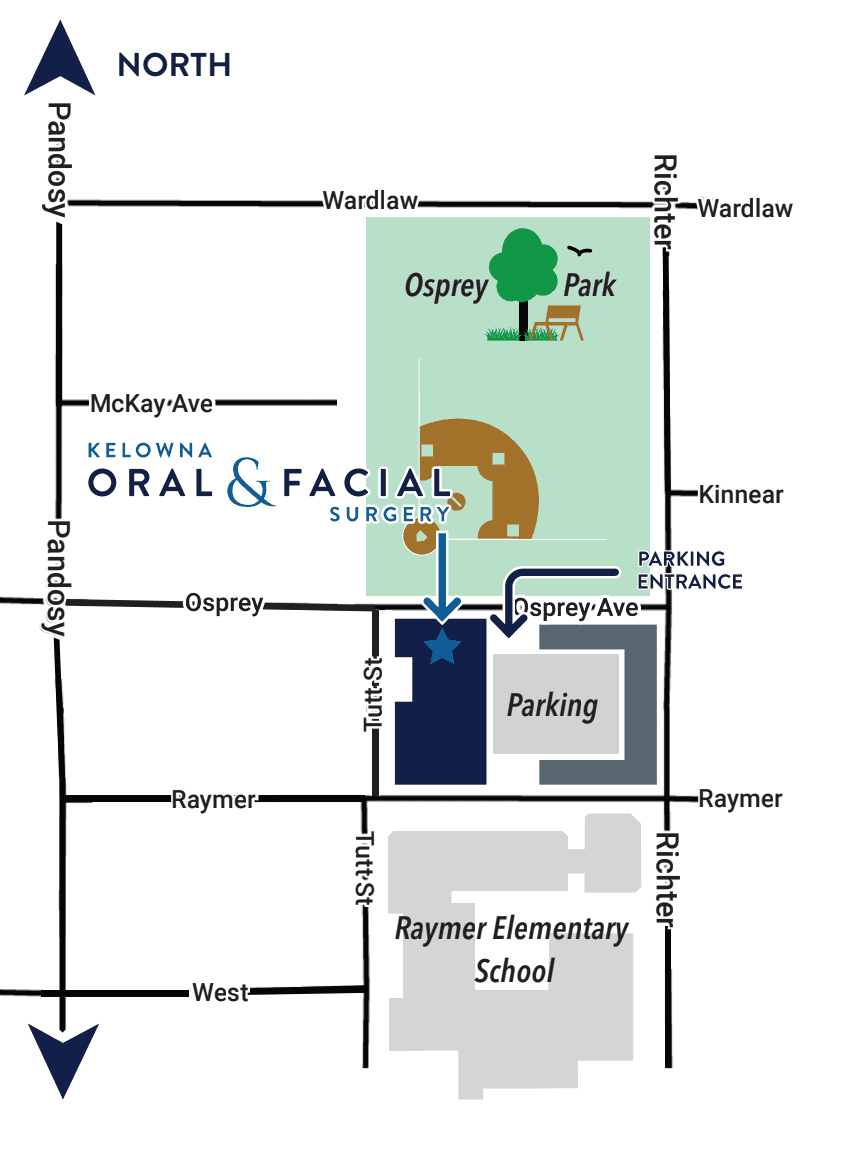
Parking Instructions
The parkade is linked to our building and the entrance to the garage is on Osprey Avenue. Please bring your license plate number with you so we can register your vehicle upon arrival.


Contact Information
Leave Us a Message
Parking Instructions
The parkade is linked to our building and the entrance to the garage is on Osprey Avenue. Please bring your license plate number with you so we can register your vehicle upon arrival.
Contact Information
Leave Us a Message
Parking Instructions
The parkade is linked to our building and the entrance to the garage is on Osprey Avenue. Please bring your license plate number with you so we can register your vehicle upon arrival.
Copyright © 2026 Dr. Scott T. Martyna, DMD, MHA, FRCDC, FACS, & Dr. Gordon Wong, DMD, FRCDC, Dip ABOMS Certified Specialists in Oral & Maxillofacial Surgery. All rights reserved.
Kelowna Oral & Facial Surgery is locally owned and operated by Dr. Martyna and Dr. Wong Dental Inc.
Copyright © 2026 Dr. Scott T. Martyna, DMD, MHA, FRCDC, FACS, & Dr. Gordon Wong, DMD, FRCDC, Dip ABOMS Certified Specialists in Oral & Maxillofacial Surgery. All rights reserved.
Kelowna Oral & Facial Surgery is locally owned and operated by Dr. Martyna and Dr. Wong Dental Inc.
Copyright © 2026 Dr. Scott T. Martyna, DMD, MHA, FRCDC, FACS, & Dr. Gordon Wong, DMD, FRCDC, Dip ABOMS Certified Specialists in Oral & Maxillofacial Surgery. All rights reserved.
Kelowna Oral & Facial Surgery is locally owned and operated by Dr. Martyna and Dr. Wong Dental Inc.