Kelowna Oral
& Facial Surgery
Kelowna Oral
& Facial Surgery
Kelowna Oral
& Facial Surgery
We are a modern oral & maxillofacial surgery clinic, dedicated to providing advanced surgical care in a comfortable and compassionate environment.
We are a modern oral & maxillofacial surgery clinic, dedicated to providing advanced surgical care in a comfortable and compassionate environment.
We are a modern oral & maxillofacial surgery clinic, dedicated to providing advanced surgical care in a comfortable and compassionate environment.

Certified Specialists in Oral & Maxillofacial Surgery







About Us
Environment
Environment
Kelowna Oral & Facial Surgery is a team of experienced, allied health care professionals and support staff. Our surgical team consists of certified specialists in Oral & Maxillofacial Surgery, Certified Dental Assistants who are surgically and sedation trained, and Registered Nurses who apply their extensive medical training to the comfort and safety of our patients.
Kelowna Oral & Facial Surgery is a team of experienced, allied health care professionals and support staff. Our surgical team consists of certified specialists in Oral & Maxillofacial Surgery, Certified Dental Assistants who are surgically and sedation trained, and Registered Nurses who apply their extensive medical training to the comfort and safety of our patients.
Our administrators will provide you with the information needed prior to a consultation visit, a surgical visit, and any subsequent follow-up appointments. Our entire team is dedicated to making your entire surgical experience safe and comfortable.
Our administrators will provide you with the information needed prior to a consultation visit, a surgical visit, and any subsequent follow-up appointments. Our entire team is dedicated to making your entire surgical experience safe and comfortable.


Technology
Technology
Kelowna Oral & Facial Surgery utilizes carefully selected, and clinically-proven, modern technology to facilitate treatment. Digital x-rays and scans, along with digital treatment planning of implants and corrective jaw surgery allow us to achieve optimal outcomes. Cutting edge technology streamlines individual treatment plans, and improves outcomes.
Kelowna Oral & Facial Surgery utilizes carefully selected, and clinically-proven, modern technology to facilitate treatment. Digital x-rays and scans, along with digital treatment planning of implants and corrective jaw surgery allow us to achieve optimal outcomes. Cutting edge technology streamlines individual treatment plans, and improves outcomes.
Our Facility
Our Facility
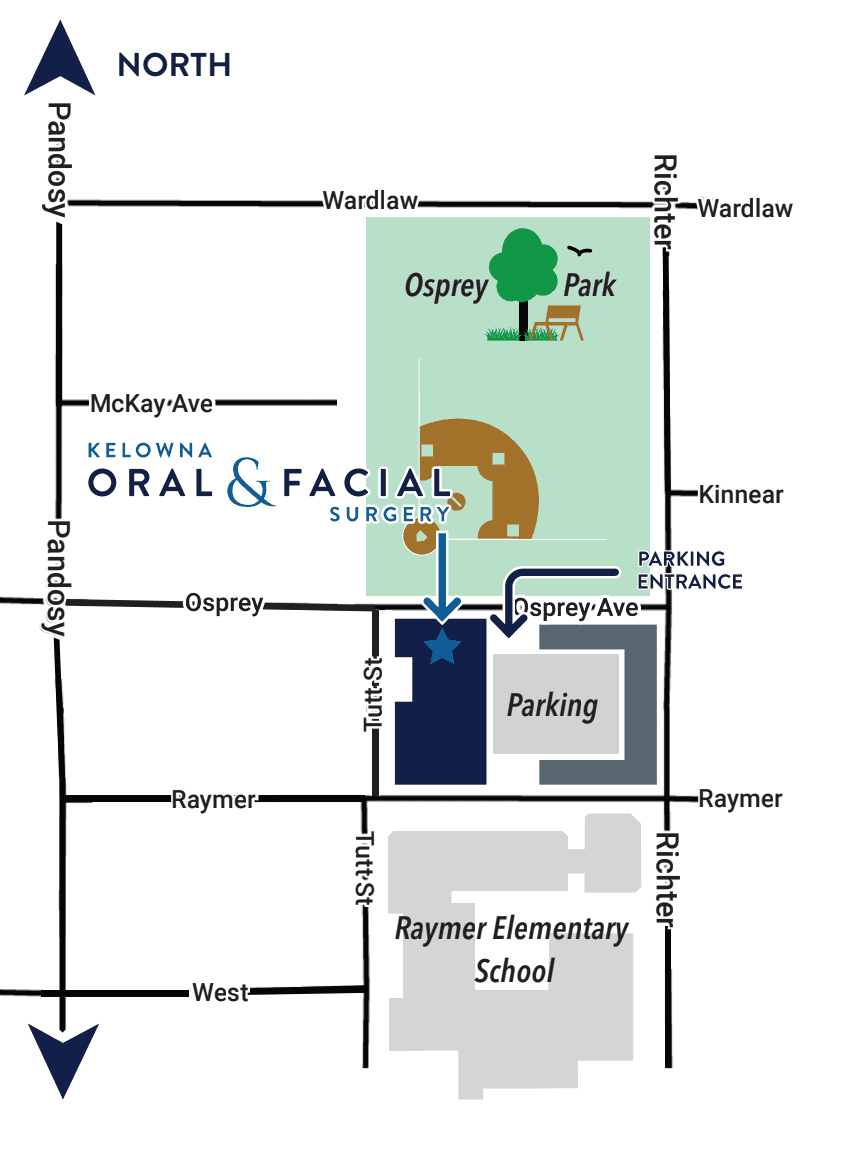
Kelowna Oral & Facial Surgery is a modern oral and maxillofacial surgery facility, which includes consult rooms, patient treatment rooms, and operating rooms for surgeries performed under general anesthesia. There is also a conference room where our surgeons provide lectures to the local dental and medical community. Our facility is conveniently located in the South Pandosy district of Kelowna, near the hospital. There is ample free parking available on-site in the attached parkade (entrance off of Osprey Avenue).
Kelowna Oral & Facial Surgery is a modern oral and maxillofacial surgery facility, which includes consult rooms, patient treatment rooms, and operating rooms for surgeries performed under general anesthesia. There is also a conference room where our surgeons provide lectures to the local dental and medical community. Our facility is conveniently located in the South Pandosy district of Kelowna, near the hospital. There is ample free parking available on-site in the attached parkade (entrance off of Osprey Avenue).


Community
Community
Kelowna Oral & Facial Surgery provides outstanding care and attention to the patients of our kind referrals. Our team works together with referring dentists, denturists, and physicians with a patient-centered philosophy. We consider it our privilege to be a part of your treatment, and to be a trusted consultant for your regular care provider. We are actively involved in the local dental and medical communities and are fortunate to work alongside such incredible care providers.
Kelowna Oral & Facial Surgery provides outstanding care and attention to the patients of our kind referrals. Our team works together with referring dentists, denturists, and physicians with a patient-centered philosophy. We consider it our privilege to be a part of your treatment, and to be a trusted consultant for your regular care provider. We are actively involved in the local dental and medical communities and are fortunate to work alongside such incredible care providers.
Kelowna Oral & Facial Surgery is a small, locally owned and operated clinic. We are proud to provide a stimulating and meaningful work environment for our valued employees, and the best possible care for our patients.
Kelowna Oral & Facial Surgery is a small, locally owned and operated clinic. We are proud to provide a stimulating and meaningful work environment for our valued employees, and the best possible care for our patients.
About Us
About Us





Satisfied Clients
Satisfied Clients
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Michelle MacArthur
We had a wonderful experience with Kelowna Oral and Facial Surgery when a member of our family had their wisdom teeth removed. From start to finish, the entire process was smooth, professional, and thoughtfully supported. The staff were kind, calm, and attentive every step of the way — which made a big difference in helping us feel at ease.Perhaps most helpful for anyone hesitant is that when our family member came out they gave a thumbs up and one of the first things they said was, "Mum, they deserve a 5 star review."
Jenna Findlay
I don’t have anything but raving reviews for the whole team at Kelowna Oral & Facial Surgery. I had 4 wisdom teeth extracted today and was feeling nervous, to say the least. From the moment I arrived, I was given the most exceptional care I’ve ever experienced.The receptionists were friendly and warm. The whole team was phenomenal and eased all my anxieties. Marlee, you are such a delight! I’ve never had someone get an IV in as quickly as you. You’re a true ray of sunshine. And Dr. Wong, you are an exceptional surgeon and I couldn’t have trusted my care in anyone else’s hands. Thank you for everything to this amazing team!!!!
Gail Smith
I recently had an oral surgery with Dr. Wong to remove my mandibular bone Tori from my lower inside and outside jaw. Dr. Wong clearly advised me what this procedure entailed and the recovery time involved for the sutures to dissolve in my gums. The large operating room in the back was very impressive with RN's and an Anesthesiologist who sedated me so seamlessly and I felt no nausea when I woke up. Your entire staff showed me so much care and concern. Dr. Wong personally called me a day after my surgery to make sure I was recovering ok and asked if I had any questions. Nice personal touch. Thanks Dr. Wong and Team.
Sheila Cederholm
Dr. Wong and the entire staff were outstanding when I went in to have oral surgery. I was quite emotional and they all made me feel at ease. Would recommend this office for all oral and dental work. Thank you all so much.
Lauren Aitchison
Dr Martyna and the entire staff were absolutely amazing from Start to finish. I had all 4 of my wisdom teeth out this week and have been so impressed with their professionalism, kindness and care. From the front of house to team, to the nurses and support staff and Dr Martyna himself. Felt so wonderful to be in such good hands, especially with the pre conception of having wisdom teeth out. Thanks again to you all :)
Mike Soloshy
I had an upper plate denture for about 42 years but I was never happy with the discomfort and pain from them. Dr Wong was able to install surgical implants and together with Dr. Zeng at Capri Dental I now have a great set of teeth again. I highly recommend Dr Wong and Kelowna Oral Surgery. My experience with them could not have been better.
Contact Information
Leave Us a Message
Parking Instructions
The parkade is linked to our building and the entrance to the garage is on Osprey Avenue. Please bring your license plate number with you so we can register your vehicle upon arrival.


Contact Information
Leave Us a Message
Parking Instructions
The parkade is linked to our building and the entrance to the garage is on Osprey Avenue. Please bring your license plate number with you so we can register your vehicle upon arrival.
Contact Information
Leave Us a Message
Parking Instructions
The parkade is linked to our building and the entrance to the garage is on Osprey Avenue. Please bring your license plate number with you so we can register your vehicle upon arrival.
Copyright © 2026 Dr. Scott T. Martyna, DMD, MHA, FRCDC, FACS, & Dr. Gordon Wong, DMD, FRCDC, Dip ABOMS Certified Specialists in Oral & Maxillofacial Surgery. All rights reserved.
Kelowna Oral & Facial Surgery is locally owned and operated by Dr. Martyna and Dr. Wong Dental Inc.
Copyright © 2026 Dr. Scott T. Martyna, DMD, MHA, FRCDC, FACS, & Dr. Gordon Wong, DMD, FRCDC, Dip ABOMS Certified Specialists in Oral & Maxillofacial Surgery. All rights reserved.
Kelowna Oral & Facial Surgery is locally owned and operated by Dr. Martyna and Dr. Wong Dental Inc.
Copyright © 2026 Dr. Scott T. Martyna, DMD, MHA, FRCDC, FACS, & Dr. Gordon Wong, DMD, FRCDC, Dip ABOMS Certified Specialists in Oral & Maxillofacial Surgery. All rights reserved.
Kelowna Oral & Facial Surgery is locally owned and operated by Dr. Martyna and Dr. Wong Dental Inc.